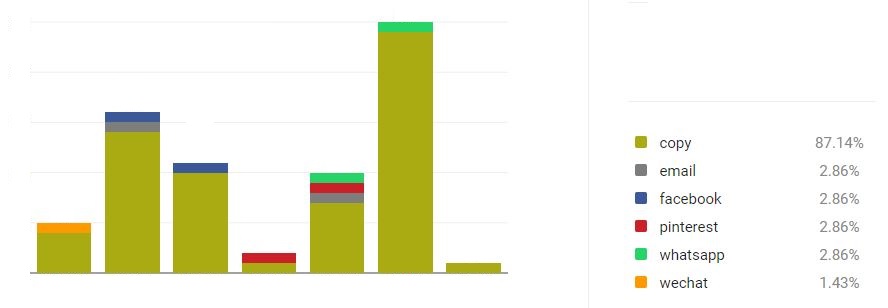
The last time we checked, 87% of our active visitors copied content from this site without acknowledgement.
This helps us know that we are doing things that interest you.
So, give us a smiley before you go.
 |
www.moyoway.com |
 Buy your Certified Organic |
|

|
|
CLICK FOR NAKED www.moyoway.com |
Moyo is an African origin word which implies that the
"heart and mind act as one to cultivate the spirit”
Is the HPV-Vaccine worth it?
>Home Page >>Vaccines >>>HPV-Vaccine
Study looks at possible ways of increasing HPV vaccination uptake
A study has just been published in Paediatrics to establish perspectives about Human Papilloma Virus (HPV) vaccine. Whilst 82% of paediatricians responded, only 56% of family physicians (FP) did.

It was found that “For 11-12 year-old girls, 60% of paediatricians and 59% of family physicians strongly recommend HPV-vaccine”. For boys of the same age it was 52% and 41% respectively. In addition, “more than one-half reported” 25% or more parents deferred the vaccination.
The study crucially found, “At the 11-12 year well visit, 84% of paediatricians and 75% of family physicians frequently/always discuss HPV-vaccination”.
However, those who occasionally / rarely discuss (18%) were more likely to :
- be family physicians
- be male
- disagree that parents will accept HPV-vaccine if discussed with other vaccines
- report that 25% to 49% of parents defer, and express concern about waning immunity
The authors concluded, “Addressing physicians’ perceptions about parental acceptance of HPV-vaccine, the possible advantages of discussing HPV-vaccination with other recommended vaccines, and concerns about waning immunity could lead to increased vaccination rates”.
This latest study does nothing to ease our concern that parents are being given sufficient information on the risks of adverse events in order to make properly informed decisions.
South African HPV-Vaccine ‘health specialist’ reprimanded by expert researcher
It’s been reported that the Cancer Association of South Africa (CANSA) will this year update their “Fact Sheet on Human Papilloma Virus Infection and Cancer” to include important research contributions by Dr Sin Hang Lee — a scientist who has done detailed research on the HPV-vaccine.
This positive outcome was brought about after a concerned female South African citizen questioned CANSA about the safety of the HPV-vaccine. The questions led to a scientific debate, between the citizen and CANSA’s Professor Herbst, during which the professor misinterpreted the work of researcher Dr Lee to deflect the concerns of the citizen.
Dr Lee himself responded to Professor Herbst, accusing him of “trying to dismiss a very important scientific issue which has affected the health of many teenagers worldwide”, and of being unqualified to do so. Dr Lee summarised saying, “To protect the health of the young children there is an urgent need for open debate of the risks versus benefits of HPV vaccination being recommended or forced onto the 12-year old school girls and boys. A simple declaration of vaccine safety made by some armchair professor like you does not serve the interest of the public”.
Professor Herbst has given an undertaking to now include Dr Lee’s counter arguments and other relevant information, and to inform himself further about Dr Lee’s other key research contributions.
A very different result to the ones we reported in November 2015 where Swedish authorities, alongside those in other countries, are doing their best to cover up any adverse data of HPV-vaccination.
November 2015 - Swedish (and Others) Cover Up
The Swedes are known for their cautious approach to public health. The Swedish authority that oversees the safety of drugs and vaccines, the Medical Products Agency (MPA), had set about upping its levels of surveillance for side effects to the highest levels when the HPV-vaccine Gardasil was unleashed on adolescent girls in 2012.

This degree of scrutiny was deemed the way to go given that GSK’s swine flu vaccine Pandemrix had previously been found to cause narcolepsy when used between 2009-10.
Emerging on Swedish radio news over recent days have been revelations by a Swedish MPA scientist, Rebecca Chandler, who had been charged with running studies to investigate the risk of one particular side effect, Postural Tachycardia Syndrome (PoTS). This is a life-altering and debilitating condition characterised by orthostatic intolerance (the development of symptoms when upright that are relieved by lying down).

Symptoms include headaches, fatigue, palpitations, sweating, nausea, fainting and dizziness and a greatly elevated heart rate when upright. A Danish study published earlier this year found that 60% of adolescent girls suffer from PoTS, the symptoms being initiated within hours of vaccination. The cluster of symptoms is increasingly being referred to among sufferers as Post-Gardasil Syndrome or PGS.
When news from Denmark revealed the extent of the PoTS cases linked temporally with Gardasil vaccination, the MPA decided, of all things, to terminate its trial. Rebecca Chandler, who was becoming increasingly convinced that PoTS was a significant side effect, objected.
But the MPA wasn’t about to change its mind. Her sense of concern and disillusionment triggered her resignation from the MPA, and she has now blown the whistle on the events, despite this news not being broadcast through mainstream media channels (typical of attempted cover-ups of this type).
We were briefed about these unfolding events by our Swedish friends at Envirohealth Mattersand felt compelled to get the story out. There’ll undoubtedly be more to report as news emerges in Sweden.
And one wonders whose health the MPA is really protecting anyway …
More on PoTS
Research is now suggesting that PoTS may be triggered by virus-like particles within the vaccine.
New reports from Denmark suggest that Sanofi Pasteur, the European manufacturer of Gardasil, have been caught understating the side effects of this vaccine to prevent it being linked to PoTS. Rather than looking at the whole range of symptoms of PoTS, the company’s data are based only on searches for ‘postural vertigo’ and ‘orthostatic intolerance’. These show up in only 26 of the 480,000 women vaccinated.
Instead, many of the other symptoms such as dizziness and fainting should have been evaluated. These results are in stark contrasts with those published in Vaccine in May 2015 which showed 60% prevalence of PoTS. It really highlights the measures that vaccine manufacturers will go to to protect their profits.
Current investment in HPV-vaccine research
In Canada, Professor Genevieve Rail from Concordia University is concluding a 4-year research grant ($270,000) to evaluate the safety and effectiveness of the HPV-vaccine.
Her conclusion was it should not be recommended and she “called for a moratorium on its use”
She said, “I’m sort of raising a red flag, out of respect for what I’ve found in my own study, and for the despair of parents who had totally perfect 12-year-olds who are now in their beds, too tired to go to school”. She added; “Yes, we’re going against the grain, and we are going against those who are believed, i.e. doctors and nurses and people in public health.”
Rail’s findings have been met with outrage from pro-vaccine quarters. “This is akin to funding research that purports to show tobacco smoking does not cause lung cancer,” charged Eduardo Franco.
A study published in 2014 in the journal Cancer Epidemiology, Biomarkers & Prevention found that 27% of physicians in America were not recommending this vaccine to the key target group of 11 and 12-year-olds. Physician recommendations were also found to be the most important reason for parents choosing vaccination for their children.
To offset this, last month saw the Boston Medical Center receive an injection of $1.04 million to improve uptake rates of the HPV-vaccines. This included education to physicians so they could engage parents in “motivational interviews” to get them onboard with HPV-vaccination to achieve the target of an 80% HPV-vaccinated population. These funds are almost 4 times the amount that Professor Rail’s group at Concordia University was awarded.
With boys now as much the target as girls, the global market for these vaccines has doubled. In the EU, the new Gardasil 9 has now been approved for boys and girls aged upwards of 9. It targets ‘high-risk’ HPV types 16, 18, 31, 33, 45, 52 and 58, as well as the ‘low-risk’ types 6 and 11, known more commonly to cause genital warts. All are sexually transmitted.
While convincing evidence of long-term efficacy of reducing cervical cancer rates is too early to call, the protective effects of the vaccine for boys are even more speculative.
A new therapeutic vaccine, GTL001, is currently going through Phase 1 trials and this focused on what we do if you do have the HPV strains 16 and 18. Currently there isn’t much in terms of treatment once these are detected. This can then be targeted at the people who need it rather than vaccinating the whole population, who don’t necessarily need it.
What can we do?
Japan, a country that is often ahead of the game in this area, withdrew its general recommendation for the HPV-vaccine in 2013 due to the concerns over the adverse reactions. They have places where those affected by vaccine related conditions can go and where the medical professionals have been educated on how to deal with them.

Guidelines include asking about “all the symptoms with details, including the quality of pain, location of the pain, the severity of the pain, fatigue, motor dysfunction, memory, and recognition. At the same time, taking care of their mental health is also important.” This is such a contrast to “motivational interviewing” the parents to get their consent or being met with ridicule in the UK and some other EU countries.
It is also crucial that adolescents, supported by their parents or families, be given the chance to opt out should the children choose to abstain from sexual activity during the early years of adolescence. This may be through choice, out of concern over the risks of vaccination on one hand, or sexually transmitted diseases including HPV on the other. There may also be other cultural or religious reasons, and these should be respected.
A survey by Cancer Research UK showed that around 20% of the target population are likely to opt out. Among the reasons given were:
- “Because I am not sexually active and will not be until I get married.”
- “My Mum didn’t think it was necessary for me to have the vaccine since I won’t be sleeping around.”
Sexual education should include details of the risks associated with HPV as well as vaccination. Those who are not sexually active should not be pressurised to be vaccinated. For every year children don’t expose themselves to the risks associated with vaccination, there is an additional year that the immune system can develop increased resilience through natural immunity, itself responsive to a healthy diet and lifestyle, as well as natural exposure to pathogens.
The following factors have been shown to cause increased risk of HPV infection:
- Early age at first sexual partner
- Multiple partners
- Smoking
- Hormonal contraceptive use
- Inconsistent condom use
In addition, to minimizing risk of HPV infection, it is also important to:
- Have regular cervical screening
- Modulate your immune system through a healthy diet and lifestyle as well as managing stress effectively
Other factors to consider:
- Vaccine manufacturers need to be made accountable for the adverse reactions, especially where efforts have been made to cover them up.
- Bureaucrats who act as accessories to such cover-ups, or who are complacent about acting on known adverse events, should equally be accountable.
- The medical profession needs to support and understand more about vaccine-damage, and ignoring it is a form of medical negligence that should be jumped on by licensing authorities.

Presently, we’re a long way from seeing action of this type, as so much of the establishment is firmly behind the principle of vaccination. Cervarix, the second common brand of HPV-vaccine, aims to be pushed hard as a single shot vaccine to overcome lower than expected take-up of Gardasil’s 3-dose schedule.
This all leaves parents and children who wish to decline the vaccine with the responsibility of understanding their right of refusal in countries where vaccines have yet to be made mandatory.
In this light, we strongly advocate you understand and support the right for informed consent in relation to vaccination, a platform being pushed by the European Forum for Vaccine Vigilance.
Don't be intimidated
If you or somebody in your family has suffered adverse effects to vaccines, we encourage you join a support group and help get your voice on the matter heard

Among these are:
- Association for HPV-Vaccine Injured Daughters (AHVID), UK or their Facebook page
- R.E.G.R.E.T (Reaction and Effects of Gardasil Resulting in Extreme Trauma), Ireland
- Gardasil Awareness New Zealand (GANZ), NZ
Credit : Alliance for Natural Health International (ANH-Intl).
What's Your Story?
Help to keep it real and tell your story.
Comments about your experiences and opinions will go a long way to helping all of us.
Comments from Other Visitors
Click the underlined and highlighted text to read the full article.
The HPV Vaccine is the most dangerous vaccine yet - WHO
Health authorities have tried their best to continue telling everyone that HPV vaccines (there are three different types available) are safe, despite …



Look Around
|
Home |
Causes |
|
Site Map |
Search |
|
Latest Pages |
RSS Setup |
|
Google+ |
Facebook |
|
Twitter |
Pinterest |
|
Help |
Downloads |
|
Contact Us |
About Us |
Recent Articles
-
Naked Organics, Organic Infusions and Tisanes
Naked Organics is Moyofarm's retail brand to buy highly nutritive certified organic foods at wholesale prices via Amazon EU -
Submission for Fu-Qu Competition from MM Cosmetica #2
We don't believe that natural products should come at a premium. It suggests that products produced with chemical additives is now normal. That sounds -
GMO Food information that you will not find in mainstream media
GMO Food is the rosy looking oversized bright red strawberry on the shop shelf, but, behind the strawberry is an unproven science that is NOT "substantially equivalent" nor a food material that your g…
Sage Advice

Avoid advertising in every possible way. Inform yourself and you will always find exactly what you are looking for
Safer Ecosystem

For the sake of a safer user and advertiser ecosystem, this website is Google Ad Free
|
|

Top of Page |
Enjoy this page? Click & share using the icons below
|
Global |
Site |
Search |
Latest |
Help |
Downloads |
Contact |
About |
Enjoy this page? Click & share using the icons below
Love life, live well, keep it real and trust your own common sense!
Motivate yourself with the 4 system properties of agroecosystems: productivity, stability, sustainability and equitability
© Copyright www.moyoway.com, 2011 - 2018, Click here for Disclaimers, Copyright & Terms of Use, Author - Marcel Blankenstein